What Is Ptosis (Blepharoptosis)?
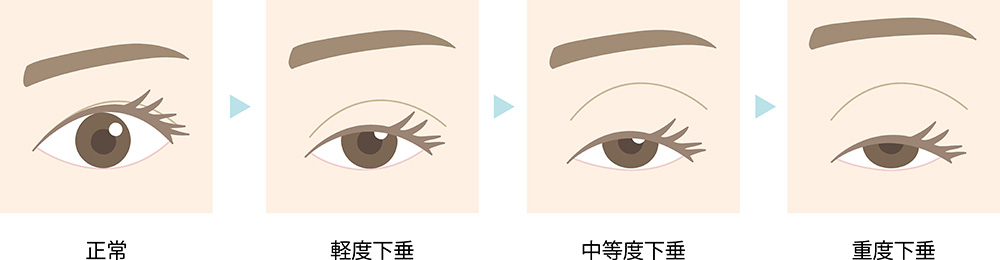
Ptosis is a condition in which the upper eyelid droops and may cover part of the pupil, making the upper field of vision difficult to see.
The most common cause is weakening, stretching, or partial separation of the levator aponeurosis—the tendon-like tissue where the eyelid-lifting muscle attaches.
Less commonly, ptosis is congenital, due to under-function of the eyelid-lifting muscle from birth, which can sometimes affect visual development.
Symptoms include not only reduced vision in the upper visual field, but also forehead strain from unconsciously lifting the eyebrows to see better.
This may lead to forehead wrinkles, headaches, or shoulder/neck tension.
In appearance, the eyes can look “sleepy” or tired.
Types of Ptosis
Ptosis can be broadly divided into three types:
- Congenital ptosis (myogenic ptosis)
- Acquired ptosis (aponeurotic ptosis) – develops in adulthood
-
Pseudoptosis – the eyelid looks low, but the muscle and tendon are normal
Congenital Ptosis (Myogenic Ptosis)
Some people are born with ptosis.
Most cases are simple congenital ptosis, in which the levator muscle does not develop normally and is replaced in part by firmer fibrous tissue.
Eye movements are usually otherwise normal, but when only one eye is affected, it can interfere with visual development; early treatment may be necessary.
Acquired Ptosis (Aponeurotic Ptosis)
This is the most common form in adults, often related to aging.
It is also more likely in people who have worn hard contact lenses for many years or who have had previous eye surgery.
In this type, the eyelid-lifting muscle itself is normal, but the aponeurosis attaching the muscle to the eyelid becomes stretched, thinned, or partially detached.
Pseudoptosis (Dermatochalasis-related)
In pseudoptosis, the eyelid muscle and aponeurosis are normal, but excess or lax upper-eyelid skin makes the lid appear low.
When the patient actively lifts the lid, it raises appropriately, confirming that the muscle function is intact.
Treatment for Pseudoptosis
In pseudoptosis, since there is no abnormality in the eyelid muscles or tendons, treatment is performed according to the underlying cause.
- Excess Eyelid Skin (Dermatochalasis)
If drooping is caused by sagging skin due to aging, excess skin is surgically removed to improve the eyelid contour. - Brow Ptosis
When the eyebrows droop because of facial nerve palsy, surgery is performed to elevate the brow and restore symmetry. - Blepharospasm
This is a condition in which the eyelid-closing muscles contract excessively, making it difficult to open the eyes.
Treatment may include botulinum toxin (Botox) injections or eyelid surgery.
If the cause is related to an aneurysm or other neurological disorder, appropriate medical treatment for that condition is also required.
Surgery for Ptosis
In most cases, ptosis is treated surgically, and the procedure is performed by a specialist in oculoplastic or reconstructive surgery.
Repair of the Levator Muscle or Aponeurosis
When the area where the eyelid-lifting muscle attaches becomes weak or detached, it is reinforced or reattached to restore normal eyelid movement.
- Incisional Approach (External Levator Advancement)
A small incision is made along the natural eyelid crease, allowing the surgeon to access and tighten the levator muscle or aponeurosis.
This method leaves a minimal scar, hidden in the eyelid fold, and can also remove excess skin at the same time.
Frontalis Suspension (“Sling”) Surgery
When the levator muscle is severely weak or there is nerve paralysis, a frontalis suspension (sling surgery) is performed.
In this method, a tunnel is created between the eyebrow and eyelid, and a thin strip of synthetic material or fascia (connective tissue) is placed to connect the eyelid to the forehead muscle (frontalis), which helps lift the eyelid.
This technique is effective but may not be suitable for children or for patients who cannot undergo local anesthesia.
Day Surgery for Ptosis
At our clinic, ptosis surgery is performed on an outpatient (day-surgery) basis, allowing patients to return home the same day.
The procedure itself is relatively short, and most patients recover quickly, though healing time may vary depending on individual conditions.
Below is the general flow of day surgery at our clinic.
Preoperative Preparation (Consultation & Examination)
- Consultation and Counseling
Before surgery, you will have a consultation with an ophthalmologist or plastic surgeon.
The doctor will explain the condition of your eyelids, the surgical method, and any potential risks or precautions. - Preoperative Examinations
Tests such as visual acuity, eyelid muscle strength, and nerve function are performed.
In some cases, blood tests or imaging studies may also be required to ensure safety. - Pre-surgery Instructions
You may be advised to avoid alcohol or heavy meals the day before surgery, and to pause certain medications if necessary.
On the Day of Surgery
- Anesthesia
The procedure is performed under local anesthesia.
A small amount of anesthetic is injected around the eyelid so that you feel no pain during surgery. - Surgical Procedure
The surgeon makes a small incision in the upper eyelid to tighten or repair the levator muscle (the eyelid-lifting muscle) and remove any excess skin if necessary.
The operation typically takes 30 to 60 minutes, though complex cases may require more time.
Postoperative Recovery
- Recovery Room
After surgery, you will rest in a recovery room for about 30 minutes to 1 hour until the effects of anesthesia wear off.
If there are no problems, you may return home the same day. - Eye Care and Cooling
Mild swelling or discomfort may occur.
Applying a cool compress helps reduce swelling and relieve pain. - Postoperative Instructions
Your doctor or nurse will explain how to care for your eyes after surgery.
Avoid rubbing your eyes, straining, or applying heat to the eyelid until advised.
Returning Home and Aftercare
- Returning Home
Most patients can go home the same day and are encouraged to rest.
Applying a cold compress for the first 2–3 days helps minimize swelling. - Medications
Antibiotics or pain relievers may be prescribed.
Take all medications as directed to prevent infection and promote healing. - Bathing and Washing
You should avoid washing your face or taking a shower immediately after surgery.
Light face washing is usually permitted after 1–2 days.
Follow-up and Monitoring
- Postoperative Checkups
A follow-up appointment is scheduled within a few days to a week to check wound healing, swelling, and signs of infection. - Suture Removal (if applicable)
If non-absorbable sutures are used, they are typically removed about one week after surgery.
Some cases use dissolvable sutures that do not require removal.
Recovery and Results
- Swelling and bruising usually improve within 2–3 weeks, but complete recovery may take up to 3 months or longer.
- Please note that this surgery is for functional improvement—it is not a cosmetic procedure.
- Minor differences in eyelid height may occur. If significant asymmetry or unsatisfactory results remain, revision surgery may be considered after swelling has fully resolved (about 3 months).
Why Both Ophthalmologists and Plastic Surgeons Are Involved
Ptosis surgery involves not only restoring visual function but also achieving a natural appearance that harmonizes with the face.
For this reason, both ophthalmologists and plastic surgeons often collaborate.
- Ophthalmologist’s Role – Functional Restoration
Ophthalmologists specialize in vision and eye movement.
They evaluate the levator muscle, nerves, and visual field, ensuring the surgery safely restores vision and eye protection. - Plastic Surgeon’s Role – Aesthetic Balance
Plastic surgeons focus on facial symmetry and soft tissue balance.
They ensure the eyelid contour looks natural, adjusting the skin, fat, and incision line for the best cosmetic result. - Postoperative Care
After surgery, both specialists work together.
Ophthalmologists monitor eye health and visual recovery, while plastic surgeons manage wound healing and scar appearance.
Our Ptosis Surgery System Plastic Surgeon

Plastic Surgeon
副島 一孝 (そえじま かずたか)
Professor and Chair, Department of Plastic and Reconstructive Surgery
Nihon University School of Medicine
Specialty Wound Healing, Regenerative Medicine, Burns, Craniofacial Surgery, General Plastic Surgery
Society Positions
- Councilor, Japan Society of Plastic and Reconstructive Surgery
- Board Member and Journal Editor, Japan Society for Burn Injuries
- Board Member, Japan Society of Surgical Techniques
- Editorial Chair, Official Journal of the Japan Society for Burn Injuries
- Delegate, Japan Society of Craniofacial Surgery
Career History
- 1988 — Graduated from the School of Medicine, University of Tsukuba
- 1988 — Joined the Department of Plastic and Reconstructive Surgery, Tokyo Women’s Medical University
- 1992 — Assistant, Department of Plastic and Reconstructive Surgery, Tokyo Women’s Medical University
- 1998-2000 — Research Fellow, University of Texas (USA)
- 2004 — Lecturer, Department of Plastic and Reconstructive Surgery, Tokyo Women’s Medical University
- 2011 — Associate Professor, Department of Plastic and Reconstructive Surgery, Nihon University School of Medicine
- 2020 — Professor and Chair, Department of Plastic and Reconstructive Surgery, Nihon University School of Medicine
Consultation and Insurance Coverage
Ptosis can cause the upper eyelids to droop and block part of your vision, affecting daily life.
This condition often progresses gradually with age and is more common among older adults.
With advances in surgical techniques, treatment can help improve the visual field in some cases.
By lifting the eyelids, surgery may help expand the field of vision and make seeing more comfortable.
Board Certifications